Med School Admissions Consulting – where excellence is the minimum.
Your potential isn’t fixed. Let’s elevate it.

Reaching your limit? Please. That’s for quitters and people who memorize bone names. We’re here to recalibrate your trajectory.
Why Choose Admissionado to Be
Your Med School Admissions Consultant Miracle Drug?
Thank you for asking.
Where do Admissionado
Med School clients get accepted?
All of the places.
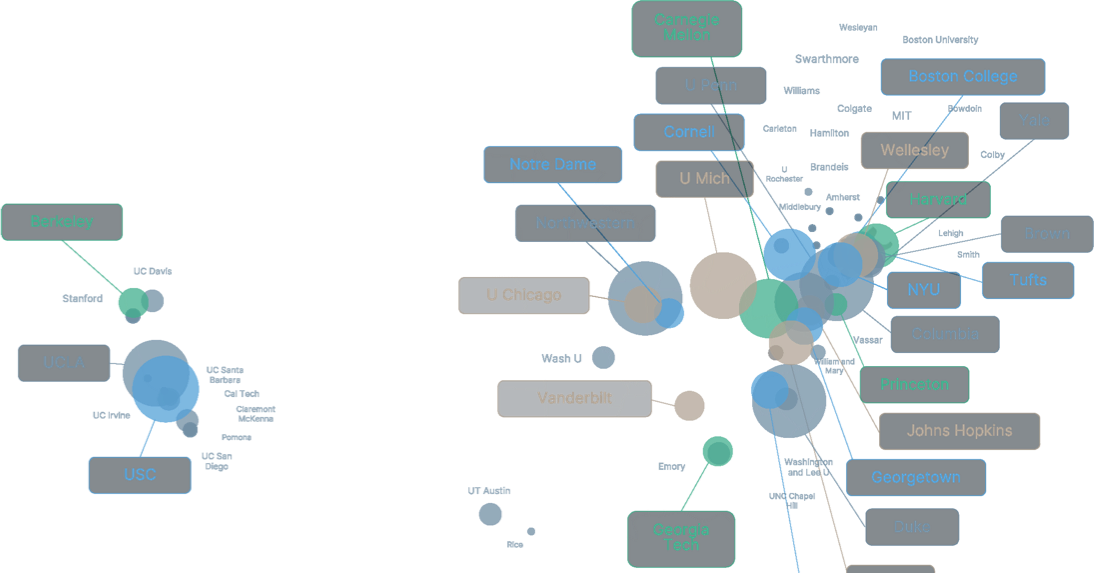
Top med schools we help you get admitted to.
School acceptance vs Admissionado acceptance.
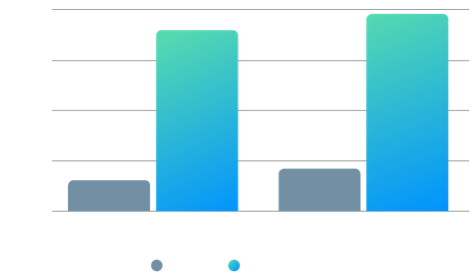
5.3x
chance of acceptance
with Admissionado

Tested and refined over decades.
Diagnosis
01The Work
02Polish
03


See the Truth
Before we build, we diagnose. We dive deep to understand your story, strengths, and ambitions—so we can craft a strategy that’s custom-fit for you. Like a brilliant diagnostician uncovering what others miss, we identify the unique markers that make your application extraordinary.
Build the Machine.
Strategy means nothing without execution. We refine, rework, and reinforce your story until it’s bulletproof. No shortcuts. Just smart, relentless iteration. Your personal statement, activities list, and secondaries won’t just be good—they’ll be surgical in their precision.
Make it Sparkle
The difference between good and exceptional? Details. We fine-tune every word, every angle, every nuance—until your application doesn’t just compete—it dominates. Med schools see thousands of future doctors. We make sure they remember you.
Med School Application Consulting Services
Ready to Apply Now
Your prerequisites are complete. Your MCAT is done. Now comes the crucial part—translating it all into an application that stands out. This service is for pre-meds ready to apply now who need expert guidance on crafting your personal statement, strategically presenting your experiences, and developing a cohesive narrative that showcases your unique path to medicine. We’ll transform your achievements into an application strategy that makes admissions committees take notice.
Select Plan Type
Primary Application
Learn MorePeripherals
Learn MoreSecondary Application Essays
Learn MoreFancy Stuff
Learn MoreEmail Support
Learn MorePhone Support
Learn MoreMed School Advanced Planning
For Folks 1 or More Years Away From Applying to Medical School
Your future medical school admission starts now. The most successful candidates don’t wait—they build clinical experiences, optimize their academic profile, and position themselves strategically long before they apply. Let’s make sure that when the time comes, your future application-self has seized every opportunity possible.
Select Plan Type
Strategy
Learn MoreMentorship Engagement
hours
A La Carte Services & Add-Ons
Purchase what you need, at your own pace, and on your own terms. We have a deep bench of A La Carte options for you to choose from.
Discovery & Competitive Edge Positioning
Learn MoreBlind 2nd Consultant Peer Review
Learn MoreLetters of Recommendation Support
Learn MoreInterview Prep (Standard)
Learn MoreInterview Prep (Premium)
Learn MoreWaitlist Support and Offer Management
Learn MoreGut Check / Rejection Analysis
Learn MorePost-Interview Reflection
Learn MoreAdmissionado Med CASPer / PREview Prep
Learn MoreMCAT Hourly Tutoring
Learn MoreHourly Support
Learn MoreWe tailor a package for your medical school journey. You can select the service level that best fits your needs and budget.
Choose Your Path
Is this worth your time?
Does partnering with an admissions consulting firm make sense for you?
I want to learn how to bring out my very best from a no nonsense but encouraging coach.
I am here because I believe that someone with better access to the competitive landscape can offer valuable perspective on what my true strengths and weaknesses are.
I have lofty ambitions, I understand the competition is fierce, and I’d like to leave nothing to chance.
I like the idea of having several folks looking at my applications, I’d love to add a professional’s insights to the mix, but I’ll keep going to solicit more and more opinions, because I’m really thorough!
I want someone to guarantee that they can help me get into my dream schools.
I’m paying a lot of money, I expect the firm or consultant I hire (who works for ME now!) to do much of the legwork. I’ll provide guidance, but it’s on YOU to tell me what to do, and when, and to keep me on track!
Full Transparency
If we’re not the right fit for you, we’ll let you know.
FAQs
Questions about our approach to Med School Consulting.
It starts well before anyone writes a word. Every engagement opens with a detailed intake built on our PULSE™ framework — a proprietary diagnostic that maps you against the five behavioral dimensions medical school admissions committees actually select for: Pioneering Spirit, Understanding, Leadership in Healing, Scholarly Depth, and Ethical Resilience. Your consultant reviews all of this in advance, forming hypotheses and identifying the threads worth pulling before a minute of live time together.
That work feeds into the strategy deep dive — the single most important block of time in the entire engagement. This isn’t a friendly get-to-know-you. It’s a strategic excavation. We test narrative hypotheses live, probe for angles you haven’t considered, and pressure-test which combinations of clinical experiences, research, motivations, and personal qualities actually produce a candidacy that stands apart. We’re also benchmarking competitiveness across tiers of programs — mapping where you realistically sit — and beginning to shape the core argument that will drive every downstream decision.
All of that gets synthesized into a Med School Action Plan: a document that captures your brand positioning, narrative themes, key differentiators, flagged concerns, school-selection logic, and a working timeline. Think of it as the architectural blueprint that keeps strategy tethered to a clear end goal.
Then comes execution — and in med, execution happens in two distinct phases. Phase one is the primary application. Your personal statement moves through our Exhaustive Iterative Drafting Process, typically four intense rounds. Early drafts are intentionally raw; we want the unfiltered version, not the polished performer. Over successive rounds, we locate the core argument, build structure, refine voice, and polish to submission-ready. Your lead consultant provides strategic direction throughout while a dedicated essay specialist works at the sentence level — two expert perspectives fused into unified feedback at every round. We also review your AMCAS, TMDSAS, or AACOMAS application and activity descriptions to ensure the full primary package tells a coherent story.
Phase two is the secondary sprint. Once schools respond with their prompts — often in waves, often with tight turnaround expectations — we apply the same iterative drafting process to each school’s essays, calibrated to that program’s specific culture, values, and how we know their committee reads. This is where volume hits, and where strategic coherence across ten, fifteen, or twenty schools either holds together or falls apart. Depending on your tier, we also cover letters of recommendation guidance, CASPer/PREview preparation, interview prep, waitlist strategy, and post-decision support.
The system is designed so that by the time you submit — primary and secondaries — you’re not just hoping the application works. You know why it works, because every element was built against a coherent argument, not assembled piecemeal under deadline pressure.
Both — with one clear point of accountability.
Every candidate is paired with a lead consultant who owns the relationship, the strategy, and the positioning from intake through decision day. That person is your quarterback. You’re not bouncing between voices or reconciling conflicting opinions about who you are and what your application should say.
Behind the scenes, your consultant works closely with a dedicated essay specialist who focuses on writing at the sentence level. We separate these roles deliberately. By splitting strategy and execution, you get depth on both: strategic thinking that isn’t diluted by line edits, and writing craft that isn’t compromised by someone trying to hold the entire arc in their head at once. This matters especially in med, where the writing workload — personal statement, activity descriptions, ten to twenty secondaries, diversity essays, addenda — is heavier than in any other vertical.
Your primary interaction is always with your lead consultant. The essay specialist’s work happens in concert with that direction, not independently. You won’t receive conflicting feedback or feel like you’re managing multiple relationships. One unified vision, executed by a coordinated team.
At Gold and Platinum, additional expert perspectives enter at specific, high-leverage moments. Blind second-consultant peer review stress-tests your materials with fresh eyes. At Platinum, MD expert consultation brings a practicing physician’s perspective into your strategy, and the Adcom Simulator models committee-style evaluation using anonymized candidate comparisons. In every case, your lead consultant integrates that input into a single, coherent direction. More signal, not more noise.
The short answer is chemistry — because in our experience, that’s what most reliably drives outcomes.
Matching based on clinical specialty interest or undergraduate background can make sense for a younger firm with less experienced consultants. At our level, it matters far less. Every consultant on our roster knows the schools, applicant archetypes, and strategic terrain cold. What varies isn’t expertise; it’s working style. The question isn’t “who knows your background,” but “who will think best with you.”
We look at communication style, temperament, intensity, and how you’re likely to engage in a high-stakes, iterative process that — in med especially — can stretch across months of sustained work from primary through secondaries through interviews. When the fit is right, everything moves faster and sharper.
We’re confident making those calls because of how we recruit. Our screening process is blind — we evaluate work product with no résumé attached — and roughly 5–6% of applicants make it through. The result is a roster where every consultant clears what we call the VIP bar: we could assign any one of them, sight unseen, to the highest-stakes engagement we’ve ever taken on and feel completely comfortable. That’s not aspirational language. It’s the standard we enforce.
One note specific to med: some of our consultants are physicians or current residents. Some are not. We address this in more detail elsewhere, but the short version is simple — your primary consultant is selected for excellence at this job, and every engagement also includes strategic input from an MD who is actively inside the system. You’re covered on both fronts, regardless of who leads.
Our standard turnaround is 72 hours from the time a draft lands in our inbox. That applies to every round of the Exhaustive Iterative Drafting Process — personal statement, secondaries, diversity essays, addenda — from the first raw pass through final polish.
In practice, it’s often faster. But we quote 72 hours deliberately. We’d rather set a realistic expectation and overdeliver than promise a flashy 24-hour turnaround and return feedback that hasn’t had time to do its job. Speed without insight is noise. A rushed edit that misses the structural problem in your second paragraph isn’t fast — it’s a wasted round.
Here’s what’s actually happening inside that window. Your lead consultant reads the draft at altitude — usually soon after it arrives — evaluating it the way an admissions reader would: what’s landing, what’s missing, and where the argument needs to go. That strategic guidance is then handed to the essay specialist, whose job is to go deep: line by line, sentence by sentence, tightening logic, refining voice, and pushing execution to match the strategy. By the time the draft comes back to you, you’re seeing two expert perspectives fused into a single, unified set of feedback. That collaboration is the point — and it’s not something you want rushed.
One practical note that matters more in med than anywhere else: turnaround speed is partly in your hands, and during the secondary sprint it becomes critical. Schools send prompts in waves, often expecting responses within two weeks. When drafts come back promptly, we can maintain momentum. When gaps appear, the backlog compounds fast. The candidates who navigate secondary season best treat it as a sustained sprint — and match our rhythm.
Yes — all of them. Every background, every profile type, every competitive starting position.
This is one of the biggest differences between us and many firms that market themselves as “the best.” We work with candidates holding elite MCAT scores who need help telling a story that isn’t forgettable, and candidates below the median at their target schools who need careful, intelligent framing. Post-bacc students rebuilding an academic record after a first career. Career changers whose path to medicine isn’t linear or obvious. Nontraditional applicants who are older, took gap years, or came to medicine through unconventional routes. Candidates with institutional action or academic integrity concerns that need to be handled with precision and zero panic. International medical graduates navigating a system that wasn’t designed with them in mind.
We don’t cherry-pick clients to protect a marketing statistic. That’s worth saying plainly, because it’s common in this industry and almost never acknowledged. When a firm quietly turns away candidates with real risk and then advertises pristine success rates, that number isn’t measuring consulting quality — it’s measuring intake selectivity. When you have the skills to do this work well, you don’t need to screen for safety.
That said, we’re honest about what’s realistic. If your MCAT and GPA profile is significantly misaligned with your target list, we’ll say so — not to cap ambition, but to ground the strategy. Sometimes that means retaking the MCAT. Sometimes it means considering DO programs alongside MD targets. Sometimes it means taking a gap year to strengthen clinical hours or research. Our job isn’t to co-sign fantasy lists; it’s to build smart portfolios with real reaches, credible targets, and well-chosen safeties. Often, the most valuable thing we do is tell you the truth you’re not hearing elsewhere.
The candidates who thrive with us share one trait that has nothing to do with stats or pedigree: they’re coachable. They engage, they reflect, and they’re willing to be pushed past what’s comfortable. If that’s you, the rest is our job.
Earlier than feels urgent — and almost certainly earlier than you think you need to.
The single strongest pattern we’ve observed across thousands of med school candidates and nearly two decades is this: earlier engagement produces stronger outcomes. Not marginally. Meaningfully. And the reasons are mechanical, not philosophical.
A candidate who engages in the winter or early spring before their application cycle has time to do the foundational work properly — PULSE™ diagnostic, competitive benchmarking, narrative positioning, personal statement pre-flight, activity description strategy — without the entire process collapsing into a panicked sprint. They test narrative hypotheses. They iterate. They make strategic decisions about the school list with real data, not gut instinct under pressure. By the time AMCAS opens in May, they aren’t inventing a story. The story already exists because it’s been thought through with direction.
For Advanced Planning candidates — those still completing prerequisites, building clinical hours, or a year or more out from applying — the leverage is even greater. You have time to shape the inputs: deepen clinical exposure, strengthen research involvement, approach MCAT prep strategically, choose recommenders deliberately, and build a profile that makes the eventual application argument feel inevitable rather than forced. Medical school admissions evaluates trajectory more rigorously than any other professional program. The earlier you build with intention, the less you have to explain or compensate for later.
For application-cycle clients, January through March before your target cycle is ideal. That window allows time for discovery, strategy, and a polished primary application ready to submit the moment the cycle opens — which matters, because many medical schools operate on rolling admissions. Earlier submission with stronger materials is a real competitive advantage, not a cosmetic one.
By late spring, we can still add value — but the runway shortens and timelines compress. By summer, when secondaries begin arriving, anyone without a solid foundation is already in triage mode.
One constraint that catches people off guard: consultant capacity is finite and fills predictably. We don’t overload rosters, because overloaded consultants do worse work — and in med, where the secondary sprint demands sustained intensity across months, roster management isn’t optional. Candidates who wait until April or May aren’t choosing between equal options — they’re choosing from what’s left.
The consultation call is free and commits you to nothing. If you’re weighing the decision, having the conversation earlier expands your choices. Waiting never does.
We use what we call the Echelon approach — and it reframes how most candidates think about school selection.
Forget precise rankings. The difference between a school ranked #8 and one ranked #15 is largely meaningless in terms of the physician you’ll become, especially once you factor in match outcomes for your target specialty, clinical training quality, location, research opportunities, and financial aid. What matters is the tier, or echelon. Within a given echelon, schools are functionally equivalent in reputation, training quality, and long-term outcomes. The distinctions between echelons can be real under specific pressure tests; distinctions within them are mostly noise.
This reframing simplifies the most anxiety-producing decision in the process. When decisions arrive, the logic is clean. Identify the highest echelon where you hold at least one admit. If you have multiple offers within that echelon, you can’t make a bad choice — decide based on specialty match data, rotation structure, location, financial package, or gut instinct. The echelon has already done the heavy lifting.
Working backward from that principle, we benchmark where your profile truly sits — the highest echelon where admission odds are meaningfully favorable given your MCAT, GPA, clinical hours, research, and overall narrative. One level below becomes safety territory. One level above is the first reach tier. From there, we build the portfolio: protect the floor, load the middle, and reach as high as ambition and profile justify.
Med school lists tend to be longer than any other vertical — typically ten to twenty programs, sometimes more. That’s partly because acceptance rates are low and the applicant pool is enormous, and partly because rolling admissions rewards breadth when it’s strategic. But more schools doesn’t mean less rigor per school. Each secondary demands real, program-specific thinking — why this school, why this curriculum, why this community. That’s why our Gold and Platinum tiers cover ten and twenty secondaries respectively: the strategic foundation is shared, but execution has to be genuine, not recycled answers with the name swapped.
One note on MD versus DO: when an MD-only list is strategically risky, we help build portfolios that include strong DO programs without treating them as consolation prizes. A well-chosen DO program is often a better outcome than a reach-heavy MD list that produces no admits. We’d rather you end up in the right seat than spend another cycle proving a point.
We also deliberately spend the most time on the hardest schools on the list — even though doing so puts our own success metrics at risk. We’d rather compete on the difficult cases than pad numbers with programs you didn’t need our help to get into.
PULSE™ stands for Pioneering Spirit, Understanding, Leadership in Healing, Scholarly Depth, and Ethical Resilience. It’s our proprietary diagnostic framework for identifying the traits elite medical school admissions committees are actually selecting for — whether or not they describe them in these terms.
The core insight is simple. Medical schools don’t admit candidates because they scored a 520 or logged 500 clinical hours. Those are surface markers — proxies meant to signal something deeper. What admissions committees are really asking, often implicitly, is: will this person become an exceptional physician? Will they handle the intellectual and emotional demands of training? And will they ultimately serve patients, advance knowledge, and reflect well on this institution over the course of a career?
The traits that predict those outcomes aren’t transcript lines or activity counts. They’re behavioral patterns — and PULSE™ maps the five that matter most.
Pioneering Spirit: Can this candidate think beyond established protocols? Medical schools aren’t just training technicians — they’re investing in people who will advance the field. You can be academically brilliant and clinically competent without ever challenging assumptions. We look for evidence of forward-thinking — not necessarily groundbreaking research, but a pattern of curiosity and reimagining how things could work better.
Understanding: Clinical knowledge isn’t the same as empathetic depth. Can you connect with patients as human beings, not case studies? Can you grasp the social, cultural, and emotional context behind illness? Committees care deeply about this because the evidence is clear: physicians who understand patients holistically produce better outcomes.
Leadership in Healing: Medicine is hierarchical, team-based, and high-stakes. Can you lead within that structure? Can you communicate clearly under pressure, coordinate across disciplines, and make decisions when the stakes are real? This isn’t about titles. It’s about demonstrated capacity to move people toward better patient outcomes.
Scholarly Depth: Intellectual curiosity that goes beyond box-checking. When you encounter something you don’t understand, do you dig deeper or move on? Have you translated knowledge into insight? Medical schools want practitioners who will keep learning, questioning, and contributing long after the boards are passed.
Ethical Resilience: Medicine confronts moral complexity constantly — end-of-life decisions, resource constraints, conflicts between autonomy and clinical judgment. Can you reason through ambiguity without defaulting to rigid rules or convenient shortcuts? This dimension separates candidates who can navigate the hardest moments of practice from those who struggle when the stakes are highest.
We score candidates across all five dimensions using inputs from the intake questionnaire and the strategy deep-dive. The results show where you’re naturally strong and where gaps exist — and from there we build strategy in two directions. Double Down means anchoring your candidacy in existing strengths. Shore Up means reinforcing weaker dimensions through experience selection and framing before the committee notices them first.
The leverage shows up everywhere. If a profile reads as research-heavy but thin on empathetic depth, we don’t hope the committee overlooks it — we reshape the narrative across the personal statement, activities, secondaries, recommenders, and interview prep so genuine Understanding is unmistakable.
PULSE™ is designed to become invisible. Like any good framework, its value is in creating clarity and shared language early — organizing complexity into a coherent argument for admission. Once that work is done, the framework fades. But the thinking it produces is embedded in every decision, from first draft to final interview.